Effective public health is crucial for a society’s well-being. Key health metrics like nutrition, infant mortality, and life expectancy provide essential insight into a population’s health status. One of the major contributors to health disparities is the uneven access to healthcare. In India, the gap between rural and urban healthcare access is stark. While only 27% of India’s population lives in urban areas, 75% of healthcare infrastructure is concentrated there.
As of 2023, more than 900 million Indians still resided in rural areas, where health outcomes are noticeably worse than in cities. Rural communities face higher infant mortality rates, increased anemia, and lower birth weights, alongside lower immunization rates and healthcare service utilization. Women, in particular, face significant health challenges due to limited access to maternal and reproductive healthcare, cultural stigmas, and the high costs of medical services.

India’s public healthcare system is structured into three tiers: primary, secondary, and tertiary care. In rural regions, primary healthcare is delivered through subcenters, primary health centers, and community health centers, designed to serve basic health needs for populations of 3,000–5,000 people. However, rural areas fall short, with 16% fewer primary health centers and 50% fewer community health centers than the government’s recommended numbers. This shortage directly impacts health outcomes in these communities.
Rural residents account for about 86% of medical visits, many traveling over 100 kilometers to reach care, with 70-80% of medical costs paid out-of-pocket. Poverty exacerbates poor health outcomes, with rural poverty having an even more detrimental effect than urban poverty. Additionally, disease prevalence in rural areas is often underreported due to data collection challenges and the reluctance of impoverished individuals to disclose negative health information, leading to routine underdiagnosis and underreporting.
Contributing Factors
Socioeconomic Barriers
The ability to afford healthcare is a major challenge for rural populations in India. In a study conducted in Orissa, one of the country’s poorest regions, 25% of households experienced hardship financing, and 40% of those facing hospitalization, had to resort to loans or selling assets to cover out-of-pocket costs. India, despite its massive population, relies heavily on private healthcare. In 2018, private out-of-pocket payments comprised 48% of total healthcare spending, while government and health insurance contributions made up 62% of overall healthcare funding.
Lower socioeconomic status is linked to both reduced healthcare access and lower utilization of more qualified healthcare providers. This lack of access leads to underuse of preventive care, such as vaccinations, which can result in more severe health issues down the line. Ultimately, this increases healthcare costs and reduces the overall healthy lifespan of the population.
Infrastructure Challenges
A lack of well-established businesses, government branches, and organizations offering essential services contributes to significant disparities in healthcare access. While private healthcare systems in India are often better funded and known for providing higher-quality care, they are mostly concentrated in urban areas, leaving rural communities underserved. Few companies have pursued cost-effective solutions to improve healthcare access in these regions. Additionally, there is minimal infrastructure for maintaining patient health records, resulting in a lack of long-term data that hinders accurate diagnosis and tracking of patient care over time.

Healthcare funding in India is a major point of criticism. Government spending on healthcare accounts for less than 1% of the country’s GDP and is primarily allocated to urban areas, where a minority of the population resides. The issue is exacerbated at the regional level, where health financing largely depends on individual states, reflecting the socioeconomic divide between urban and rural areas.
Rural residents often travel over 100 kilometers to access medical care, navigating difficult terrain and poorly maintained roads, which discourages seeking timely treatment. Inadequate transportation and poor road conditions further complicate access to healthcare services, leaving many rural populations without the care they need.
HRH shortage
Human resources for health (HRH) play a vital role in ensuring effective and high-quality healthcare systems, which are essential for maintaining and promoting public health. HRH are responsible for implementing policies, managing healthcare processes, prescribing treatments, and delivering care. Countries with low physician densities typically face poor outcomes in life expectancy and maternal and child mortality.
According to BMC Public Health, India is one of 57 countries facing a significant HRH shortage. While the World Health Organization (WHO) recommends 44.5 doctors, nurses, and midwives per 10,000 people, India’s national density stands at 20.6 per 10,000. Although this is a marked improvement from the estimated 13.6 per 10,000 in 2005, disparities remain in the distribution of HRH across the country. Urban areas have four times the doctor density of rural regions, highlighting the uneven allocation of healthcare professionals. The availability, distribution, and quality of HRH are crucial for achieving universal health coverage (UHC) in low- and middle-income countries (LMICs) like India.
Consequences
Life Expectancy
Life expectancy is closely tied to healthcare access, as factors such as early childhood mortality, deaths from injuries, and preventable deaths among the elderly all influence a population’s average lifespan. Adequate healthcare access can mitigate these issues. Life expectancy serves as a valuable indicator of a population’s overall health.
According to BMJ Glob Health, in India, life expectancy at birth was 65.1 years for the poorest 20% of households, while it reached 72.7 years for the wealthiest 20%, reflecting a 7.6-year absolute gap and an 11.7% relative gap. Women generally had higher life expectancy at birth than men, along with smaller wealth-related disparities. Across all wealth levels, life expectancy was higher in urban households compared to rural ones. The disparity in life expectancy was most pronounced among urban men, while urban women experienced the smallest gap in wealth-related inequalities.
Low life expectancy has significant economic consequences, as shorter lifespans result in fewer productive years in specialized or skilled labor, leading to higher workforce turnover. This impedes economic development and limits the technological and societal advancements that stem from a skilled workforce.
Malnutrition

India is home to an estimated 200 million malnourished individuals, highlighting the pervasive issue of food insecurity across the country. Malnutrition is a severe health condition that can lead to fatigue, decreased productivity, poor mental clarity, and reduced life expectancy in adults. In children, it can cause lasting health problems such as stunted growth, permanent physical disabilities, infections, and even death. Among the many factors influencing childhood malnutrition, access to healthcare services plays a critical role, often surpassing per capita income in its impact. Healthcare services are vital for educating families on proper childhood nutrition and providing growth monitoring, both essential in preventing malnutrition. Without these services, the long-term health and productivity of individuals can be severely compromised, further straining the community’s economic stability.
Financial Strain
Healthcare costs are one of the primary drivers of poverty in India. The financial burden of medical expenses often pushes individuals below the poverty line. A study estimated that over 63 million people in India were driven into poverty due to healthcare expenses, representing 7% of households. This financial strain can increase stress, which in turn can worsen or lead to new health problems. Moreover, financial pressures often cause people to avoid seeking preventive care, resulting in untreated conditions becoming more serious. In rural areas, the cost of healthcare is particularly overwhelming, driving otherwise stable families into poverty and deepening the debt of those already struggling.
Maternal Mortality
Limited access to healthcare in rural India significantly reduces the availability of prenatal, postnatal, and reproductive care, which in turn lowers the chances of having skilled medical personnel present during pregnancy, childbirth, or in the event of complications. Expectant mothers often miss out on crucial maternal education and training that could be life-saving.
A community investigation into maternal mortality was carried out in a rural region of North India. Maternal deaths were identified through multiple local informants and examined by medical professionals. Out of 257 deaths recorded among women aged 15-44, 55 (21.4%) were due to maternal causes. The maternal mortality ratio (MMR) was found to be 230 per 100,000 live births. The leading causes of maternal death included antepartum and postpartum hemorrhage (18.2%), puerperal sepsis (16.4%), severe anemia (16.4%), abortion (9.1%), and obstructed labor (7.3%). The majority of these deaths occurred among women from lower socioeconomic backgrounds.

Maternal deaths not only reduce overall life expectancy but also place immense strain on young families and communities, particularly in terms of meeting basic needs. The loss of a mother severely impacts childhood development, exacerbating both psychosocial and physical health challenges for the family. For impoverished families who depend on daily labor, the death of a mother can leave children without any adult supervision, further elevating the risk of adverse health outcomes and mortality.
Practices
Targeted Development of Private Hospitals in Small to Medium-Sized Communities
Social entrepreneurs in healthcare have developed profitable ways to bring medical services directly to rural regions. Their approach focuses on establishing small hospitals in semi-urban areas near public transport hubs, scaling operations to match the needs of these communities while remaining financially viable. To address the shortage of doctors and competition from urban hospitals, these smaller facilities offer recent medical graduates senior roles, providing them with better pay and more responsibility than they might find at larger urban hospitals.
Training Local Healthcare Providers
This strategy aims to leverage untrained medical providers by equipping them to recognize and treat prevalent illnesses like pneumonia and diarrhea. Local entrepreneurs who are already providing medical services create a foundational framework for enhancing the healthcare system. The goal is to recruit, hire, or collaborate with existing rural healthcare workers, offering them essential training and supplies to boost their effectiveness, support local businesses, ensure oversight, and create referral pathways for more serious medical issues.
This method seeks to alleviate the impact of common illnesses, minimize the risks of malpractice, and enhance medical education within the communities that need it most. A notable example of this initiative is the Society for Education, Action, and Research in Community Health (SEARCH), which trains community health workers, operates mobile medical units in underserved areas, conducts research, and informs public policy, even as many community health worker programs function without government support.
Telemedicine
Telemedicine leverages electronic communication technologies to deliver healthcare services to individuals in remote locations. This advancement has the potential to bridge the gap in accessible and qualified healthcare professionals between rural and urban areas while creating new market opportunities to enhance healthcare access in rural communities. Clinicians can now monitor patients remotely, allowing central hospitals to offer intensivist services without requiring patients to leave their local hospitals.
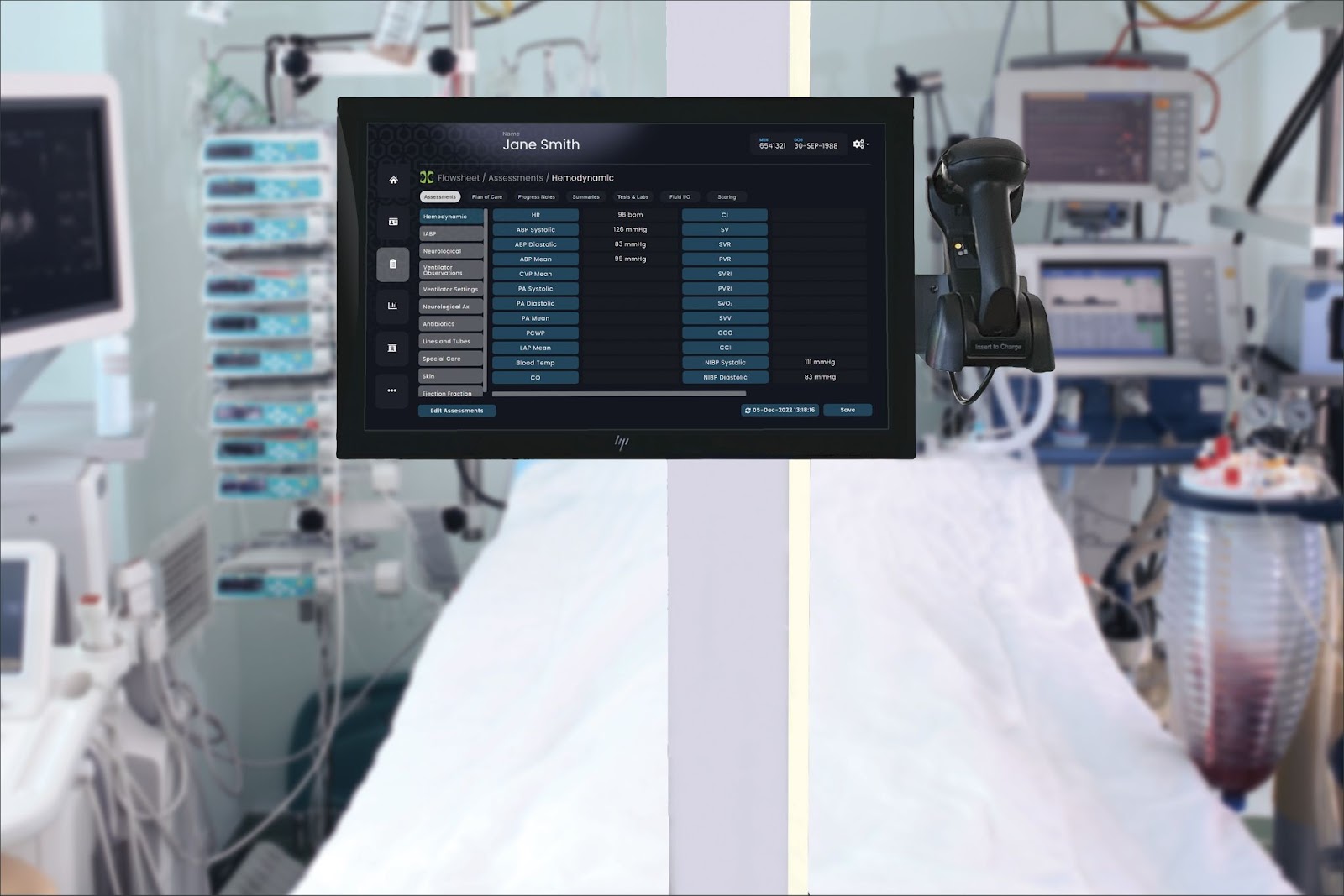
The introduction of the Clinician Assistant in Critical Care by DocBox facilitates:
- Remote connection to bedside platforms for real-time data monitoring.
- Two-way audio and video communication between the bedside Clinician Assistant and a remote PC, with pan-tilt-zoom camera controls.
- Access to any DocBox Clinician Assistant through the hospital intranet.
- Remote viewing of all bedside data, including patient demographics, care plans, and progress notes.
- Remote documentation capabilities, such as completing clinical charting, assessments, care plans, progress notes, and necessary manual entries.
- An image viewer app for accessing all PACS images.
- Access to laboratory results.
- Monitoring of physiological trends and real-time device data (excluding waveforms).
Are you ready to see how DocBox can transform your healthcare operations? Schedule your demo today and discover how our platform can enhance patient care, streamline workflows, and improve overall efficiency: https://docboxmed.com/demo/










